A 70-year-old woman presented to ED feeling unwell for 12 hrs. She was febrile and tachycardic with raised inflammatory markers (CRP 53). Her only localising feature of infection was some mild right flank discomfort earlier in the day. Urine dipstick was positive for leukocytes and a working diagnosis of pyelonephritis was made. Renal function was normal.
Her background was notable for metastatic ovarian cancer for which she was receiving palliative chemotherapy. A CT scan performed 6 weeks prior showed large, necrotic lymph node masses in the retroperitoneum.
She had presented similarly to the ED 8 days earlier and been discharged with oral antibiotics on the basis of a positive urine dipstick.
The history of retroperitoneal metastases together with recurrent UTI raised suspicion for ureteric obstruction. Diagnostic imaging was therefore required to clarify the patient’s disposition – pyelonephritis would be referred to general medicine for inpatient IV antibiotic therapy, whereas obstruction with secondary infection would be referred to urology for consideration of palliative stent or nephrostomy.
Unfortunately the patient had presented to ED during a strike by radiography staff, and CT could not be obtained until the following day.
Bedside ultrasound was undertaken to assess for signs of ureteric obstruction.
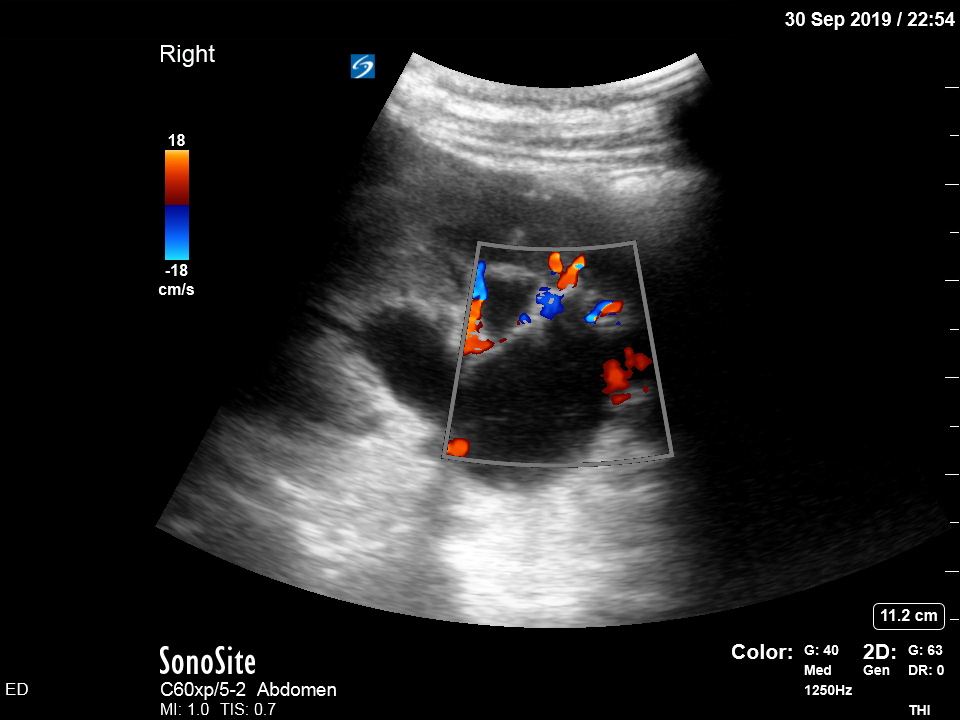

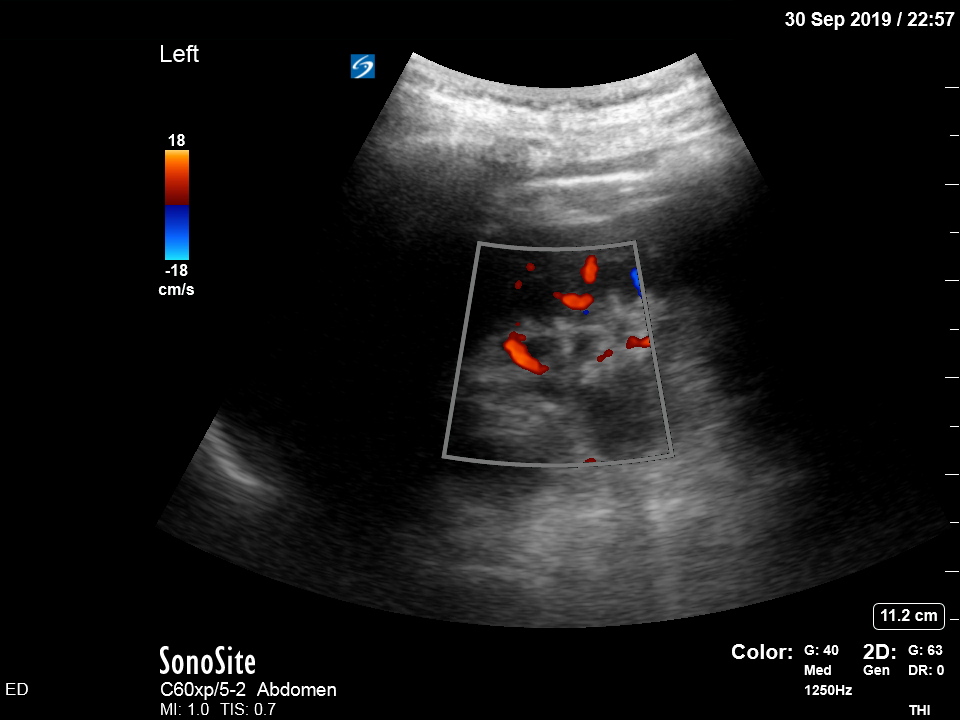
There is moderate-to-severe hydronephrosis of the right kidney. There is mild hydronephrosis on the left. Colour flow doppler is used to demonstrate that the dilated pelvis and calyces are not normal blood vessels or aneurysms.
Hydronephrosis is dilation of the renal collecting system caused by increased pressure in the ureter, strongly suggesting downstream obstruction. Possible explanations for bilateral hydronephrosis include bladder outlet obstruction and bilateral ureteric obstruction. The former is unlikely in a freely urinating patient, especially female.
The history and findings suggest that the patient has developed bilateral ureteric obstruction from progression of retroperitoneal disease.
What would have happened without POCUS?
The patient would probably have waited in ED until the strike finished and a CT could be performed. Alternatively they may have been admitted under general medicine only to later be taken over by urology after CT imaging (surgical subspecialties, generally speaking, are far less likely to accept patients with uncertain diagnoses, usually requiring imaging evidence). Such a delay to treatment could result in a dangerous deterioration in renal function.
Another (purely anecdotal) benefit of POCUS: the very ease of confirming hydronephrosis with bedside ultrasound makes the clinician more likely to consider it in the first place. At the first ED presentation, despite the history of retroperitoneal malignancy, an underlying diagnosis of ureteric obstruction was not explicitly considered and the patient was discharged – the obstruction may have already developed. Put another way, the time and effort required to obtain CT imaging (requesting the scan electronically, discussing with the radiologist, transferring the patient to and from radiology and waiting for the report) can discourage a doctor from further exploring the diagnostic possibilities, instead settling for the “easier” diagnosis of pyelonephritis (no imaging required). This is an example of premature closure bias. POCUS helps to overcome this bias by markedly lowering the threshold for engaging your diagnostic curiosity.
What was the outcome of the case?
The patient was admitted under urology. CT abdomen the next morning confirmed the ultrasound findings and revealed the cause to be progression of retroperitoneal disease. Bilateral JJ stents were placed in the operating theatre, and urine aspirate confirmed bacterial growth.
