A 50yo female presented to the ED with abdominal pain and jaundice that had developed over 1 week.
She had a background of cholecystectomy for acute cholecystitis 1 year prior. Surgery had been difficult and a post-operative MRCP* revealed stones in the cystic duct remnant – these had been managed expectantly.
On examination: haemodynamically stable, HR 68, afebrile. Jaundiced. Tender RUQ and epigastrium with no peritonitic signs. Cardiorespiratory exam unremarkable.
Blood tests (upper limit of normal in brackets):
Bilirubin 21 (20)
ALP 600 (120)
GGT 1036 (35)
ALT 249 (30)
AST 200 (30)
INR 0.9
Lipase 48 (60)
Albumin 45 (48)
WCC 5.3, neutrophils 3.7 (both normal)
Her symptoms together with obstructive LFT picture and history of cystic duct stones raised suspicion for a stone in the common bile duct (choledocholithiasis). Admitted under general surgery due to severe pain, with plan for inpatient MRCP to confirm the diagnosis prior to ERCP*.
Bedside ultrasound was performed on the ward by the surgical house officer.
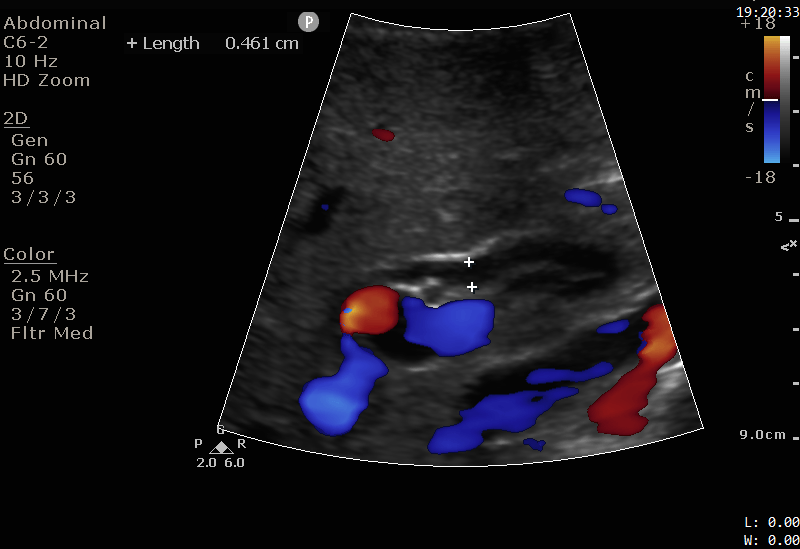
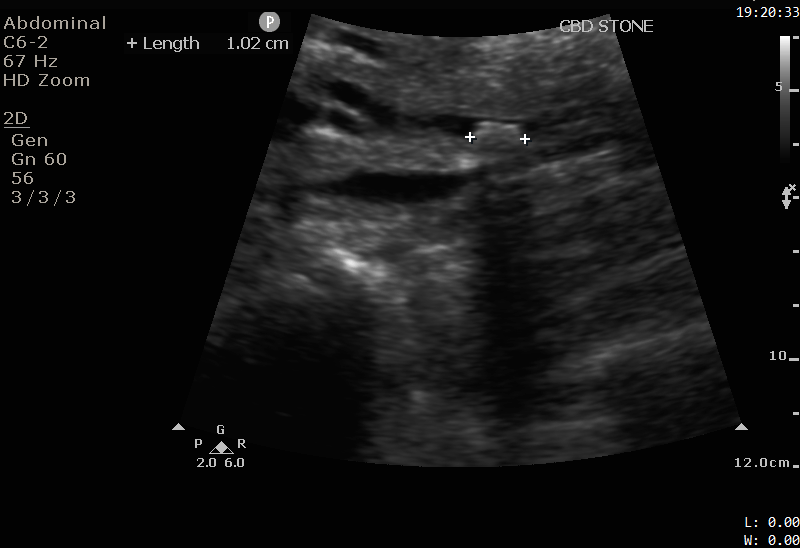

The images show a 1cm stone in the distal CBD. Note the hyperechoic (bright white) appearance, with a posterior acoustic shadow, similar to the appearance of gallstones discussed in Case 2. The CBD is not significantly dilated.
Images were shown to the radiologist. MRCP was avoided and the patient proceeded directly to ERCP.
Discussion
Ultrasound imaging of the CBD is difficult due to its small size, variable course, and frequent overlying bowel gas in the duodenum. The only ultrasound finding of choledocholithiasis may be a dilated CBD (not the stone itself), and MRCP may be performed. In this case, time and money were saved due to high pre-test probability, convincing ultrasound images and a friendly radiologist.
*MRCP (magnetic resonance cholangiopancreatography): an MRI sequence that highlights slow-moving fluid (such as bile), making it useful for demonstrating obstructions of the biliary tree such as stone, strictures or tumours.
*ERCP (endoscopic retrograde cholangiopancreatography): combines endoscopy and fluoroscopy to image the biliary tree. It is both diagnostic and therapeutic. Fluoroscopic images are generated of the CBD and pancreatic duct. Biopsies can be taken. Strictures and stones can be treated with removal or stent placement.
